Arthritis surgery includes several options designed to treat pain and loss of function caused by compartment-specific knee arthritis. Dr. Gomoll offers robotic-assisted MAKO partial knee replacement for medial, lateral, and patellofemoral arthritis, as well as the MISHA® Knee System, an implantable shock absorber designed to reduce pressure on the affected compartment while preserving the natural joint.
What is knee arthritis surgery?
Knee arthritis surgery is used to treat advanced arthritis that develops when the cartilage cushioning the joint has worn away, allowing bone to rub against bone. Although the knee functions as a single joint, it is made up of three compartments: the medial (inside), lateral (outside), and patellofemoral (behind the kneecap) compartments. Arthritis may affect one, two, or all three of these areas.
Treatment depends on which compartments are involved, the condition of the ligaments, and the patient's activity level. When arthritis affects all three compartments, a total knee replacement is often the most appropriate option.
When arthritis is limited to a single compartment and the remaining knee structures are healthy, a partial knee replacement may be a more joint-preserving alternative. For selected patients with medial compartment arthritis, the MISHA® Knee System may also be considered.
Who is a candidate for partial knee replacement or MISHA?
Partial replacement candidates have:
- Bone-on-bone arthritis confined to one compartment (medial, lateral, or patellofemoral)
- Healthy or only mildly affected other compartments — confirmed on high-quality MRI
- No symptomatic ligament instability
- An active lifestyle and the desire to retain a more natural-feeling knee
For more advanced cartilage damage that is not yet bone-on-bone, see our cartilage repair page. For meniscal-deficient knees, see meniscal transplantation.
When Partial Replacement May Not Be the Right Choice: Partial knee replacement is not appropriate for everyone. Patients with arthritis affecting two or three compartments of the knee, significant knee instability, or advanced wear in the remaining compartments are generally better candidates for total knee replacement.
Before considering surgery, conservative treatments are typically explored. These may include weight management, physical therapy, anti-inflammatory medications, bracing, and injections. Factors such as smoking, uncontrolled diabetes, and very high body weight can also increase surgical risk and may be worth addressing before elective surgery.
During your consultation, Dr. Gomoll will review your imaging, symptoms, and goals to determine whether partial knee replacement, the MISHA® Knee System, total knee replacement, or continued non-surgical treatment is the most appropriate option for your knee.
How arthritis surgery is performed
Dr. Gomoll offers three compartment-sparing options, selected by which part of the knee is affected.
Partial medial or lateral knee replacement
If decision-making confirms that only one compartment requires replacement, Dr. Gomoll performs a partial replacement of just that compartment — preserving the other compartments and the patient's own ligaments. This is generally best for patients who are more active and attuned to their knee. A partial knee replacement feels more natural than a total replacement, with better range of motion. The trade-off: the unreplaced compartments may deteriorate over time, requiring eventual conversion to a total knee replacement (typically 10–20 years later).
Dr. Gomoll uses a robotic-assisted technique (MAKO) to improve precision. A pre-op CT scan is converted to a 3D plan; the robot prepares the bone within the planned boundaries, the components are placed and cemented. Click here for more information on the MAKO partial replacement technique.
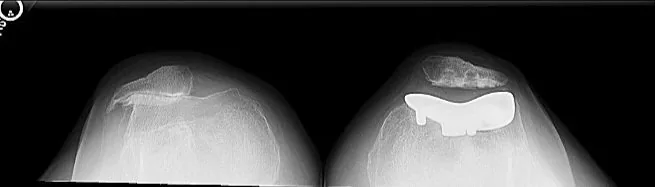
 Before
Before  After
After Patellofemoral replacement
If only the anterior (patellofemoral) compartment is arthritic, a partial replacement called patellofemoral replacement resurfaces the trochlea and patella, preserving the medial and lateral compartments and all ligaments. ABC News interviewed Dr. Gomoll on his patient being the first in the US to receive a custom patellofemoral implant for advanced patellofemoral arthritis.
Medial Implantable Shock Absorber (MISHA)
A new treatment option for medial-compartment arthritis that is symptomatic but not advanced enough for replacement. The MISHA implant — developed over more than a decade of clinical trials — is a spring-based device placed extra-articularly (outside the joint capsule) on the medial side of the knee. It absorbs load and offloads the damaged medial compartment, improving pain and function.

Recovery is faster than partial replacement — patients are typically off crutches within 2 weeks. The goal of the MISHA device is to delay knee replacement, ideally for up to a decade, after which it can be revised to either osteotomy or partial/total replacement without difficulty. Click here for further information on MISHA.
Partial replacement vs. total replacement vs. MISHA
The right operation depends on how many compartments are arthritic, the condition of your ligaments, and how active you are. Partial replacement and MISHA preserve healthy tissue when only one compartment is involved; a total replacement is the durable answer for diffuse, multi-compartment arthritis. This table summarizes the trade-offs.
| Option | Best suited for | What is preserved | Recovery pace | Typical lifespan / goal |
|---|---|---|---|---|
| Partial (unicompartmental) knee replacement — MAKO robotic-assisted | Bone-on-bone arthritis confined to one compartment with intact ACL/PCL and healthy other compartments | Your own ligaments and the unaffected compartments; feels more natural than a total | Walking same day; crutches or walker initially to help with comfort and stability, transition to cane typically within 1–2 weeks | Designed to last 10–20 years before potential revision to a total knee replacement |
| Patellofemoral replacement | Isolated arthritis of the anterior (kneecap) compartment only | Medial and lateral compartments and all ligaments | Similar to medial/lateral partial replacement | Resurfaces only the trochlea and patella |
| Total knee replacement | Diffuse arthritis affecting two or three compartments, or a deficient ACL | Resurfaces all compartments; most reliable for widespread arthritis | Similar but slower than medial/lateral partial replacement | The durable answer for multi-compartment disease designed to last 25 years or more |
| MISHA medial implantable shock absorber | Symptomatic medial-compartment arthritis not yet advanced enough for replacement, often in younger patients | The entire joint — the device sits outside the joint capsule and removes nothing | Fastest — typically off crutches within 2 weeks but rehab important to restore motion | Aims to delay replacement up to a decade; reversible by removing the implant in a simple outpatient procedure; preserves the entire knee, allowing any future intervention, including osteotomy or replacement |
Why the distinction matters: a partial replacement or MISHA leaves your own ligaments and healthy cartilage in place, which most patients find feels more like a natural knee — but those options only work when the arthritis truly is confined to one compartment, which is why Dr. Gomoll obtains high-quality imaging of the other compartments before recommending them.
Dr. Gomoll's approach to knee arthritis surgery
The central decision in arthritis surgery is how much of the knee actually needs to be replaced. For an active patient with bone-on-bone arthritis confined to a single compartment and intact ligaments, Dr. Gomoll favors replacing only that compartment — a partial knee replacement preserves the patient's own ACL, PCL, and unaffected cartilage and tends to feel more natural with better range of motion than a total replacement. To verify the diagnosis, a good-quality MRI is always obtained to assess the other compartments before a partial replacement is recommended, because the trade-off of a partial is that an unreplaced compartment can wear over time and eventually require conversion to a total.
Robotic-assisted (MAKO) technique is used to improve the precision of component positioning from a CT-based 3D plan. For younger patients whose medial arthritis is symptomatic but not yet advanced enough for replacement, the MISHA shock absorber offers a less invasive, reversible option that aims to delay definitive surgery. Dr. Gomoll has performed partial knee replacements for over 20 years and helped refine the MISHA technique through its FDA trial — see active clinical trials for related research.
Preparing for arthritis surgery
Pre-op evaluation includes standing X-rays of both knees (assessing alignment and joint-space narrowing), high-resolution MRI to confirm that the unaffected compartments are healthy, and a focused exam of ligament stability and range of motion. Standard pre-op stops apply: narcotics 14 days before, blood thinners and supplements 7–10 days before, nothing by mouth after midnight. See our before-surgery checklist.
Anesthesia & staying comfortable
Partial knee replacement is performed under spinal or general anesthesia, with long-lasting local anesthetic and occasionally also paired with a regional adductor-canal block that keeps the leg comfortable well after you wake up.
You will meet your anesthesiologist before surgery to choose the approach that fits you. A regional adductor-canal block typically lasts about 6–8 hours and is designed to preserve enough quadriceps strength to begin walking the same day. Most partial-replacement and MISHA patients are discharged the same day or after a single overnight stay, move to oral pain medication within the first day or two, and rely on it for only the first 1–2 weeks.
Worried about pain medication? The goal is a multimodal, opioid-sparing plan — the nerve block, anti-inflammatories, ice, and elevation do much of the work, so narcotics are used at the lowest effective dose for the shortest time rather than leaving you dependent on them. The full pain-control timeline is in our after-surgery instructions, and bracing and cold-therapy options are covered on our bracing & ice machine page.
Common concerns about knee arthritis surgery
"Will my insurance cover it?"
Partial and total knee replacement are established procedures generally covered when medically necessary. MISHA is FDA-cleared; coverage varies by plan and may require pre-authorization, which Dr. Gomoll's administrative team manages before surgery.
"Recovery will take forever."
Partial replacement is a faster recovery than a total — many patients are walking the same day, off the walker within two weeks, and back to recreational sport in moderation by 3–6 months. MISHA patients are often off crutches within 2 weeks.
"I'm afraid of the pain."
A regional nerve block and a multimodal, opioid-sparing protocol mean most patients report markedly less pain than the bone-on-bone arthritis they came in with. Dr. Gomoll will walk you through the plan at your consultation.
Risks to understand
Partial knee replacement and the MISHA implant have strong track records, but like any surgery they carry risks you should weigh with Dr. Gomoll before deciding. These can include infection (including periprosthetic joint infection), blood clots (DVT/PE), stiffness, implant loosening or wear over time, periprosthetic fracture, and progression of arthritis in the unreplaced compartments — which can eventually require conversion of a partial to a total knee replacement. Device-specific risks of the implants and ordinary anesthesia risks (such as nausea or, rarely, cardiac or respiratory events) are also discussed before surgery.
No knee procedure is a guaranteed permanent fix. These operations are designed to relieve pain and restore function — modern partial implants are designed to last 10–20 years — but longevity and outcome depend on which compartments are involved, alignment, body weight, activity level, and how closely you follow the rehabilitation protocol. Dr. Gomoll will review the specific risks and realistic expectations for your knee at your consultation.
Materials & technologies we use
- MAKO robotic-arm assisted system — CT-based 3D planning and intra-operative robotic precision for component positioning
- Cobalt-chromium-molybdenum femoral and tibial baseplate components with polyethylene articular surface
- MISHA implantable shock absorber — FDA-cleared spring-based extra-articular device
- Patellofemoral replacement — custom or off-the-shelf trochlear and patellar components for isolated anterior compartment arthritis
- HSS imaging — standing alignment films and 3T MRI for surgical planning
Follow-up & long-term outcomes
Partial knee replacement (MAKO)
Walking same day with walker/crutches, cane within 1–2 weeks, driving by 4 weeks (sooner for left knee), recreational sport at 3–6 months. Implants typically last 10–20 years before potential revision.
Patellofemoral replacement
Similar timeline to medial/lateral partial replacement.
MISHA
Off crutches within 2 weeks, return to most activities by 6–8 weeks. Goal is to delay definitive replacement up to a decade.
Detailed PT plans for partial replacement and MISHA are downloadable on our knee rehab protocols page. General recovery FAQs are on our after-surgery page.
Patient outcomes & press coverage
- Partial knee replacement — patient testimonial — a single-compartment arthritis patient treated with partial replacement rather than a total
- Jennifer — HTO + ACL reconstruction — a realignment osteotomy in an active patient, the joint-preserving alternative to early replacement that informs treatment selection
- ABC News — first US patient to receive a custom patellofemoral implant — press feature
- Dr. Gomoll on the Joe Rogan Experience with David Goggins — HTO discussion (alternative to early partial replacement)
- Documented intra-operative cases — cartilage and joint-preservation cases that informed treatment selection
More written outcomes are on our patient testimonials page.
Frequently asked questions
How long does partial knee replacement surgery take?
Robotic-assisted partial knee replacement (MAKO) typically takes 60–90 minutes. The MISHA medial implantable shock absorber takes about 60 minutes.
Is partial knee replacement painful?
Performed under spinal or general anesthesia, often with a regional adductor-canal block lasting 6–8 hours. Most patients are discharged the same day or next morning. MISHA recovery is more accelerated than partial replacement — patients are typically off crutches within 2 weeks.
Am I a candidate for partial vs. total knee replacement?
It depends on which compartments are arthritic. The knee has three compartments — medial (inner), lateral (outer), and patellofemoral (anterior). If only one compartment is bone-on-bone and the others are healthy, partial replacement preserves your own ligaments (ACL, PCL) and the unaffected cartilage. Dr. Gomoll always obtains a high-quality MRI to assess the other compartments before recommending partial replacement.
What materials are used?
Partial knee implants are typically a combination of cobalt-chromium-molybdenum femoral component, polyethylene tibial insert, and titanium tibial baseplate. The MAKO robot uses your CT-based 3D plan for precise component positioning. The MISHA implant is a small spring-based device placed extra-articularly to offload the medial compartment.
How long does a partial knee replacement last?
Modern partial knee implants are designed to last 10–20 years before potentially needing revision to a total knee replacement; longevity depends on activity, weight, and individual factors. During that time they tend to function more naturally than total replacements — in moderation, most patients can return to tennis, skiing, golf, and gym activities.
Is partial knee replacement outpatient or inpatient?
Robotic-assisted partial knee replacement and the MISHA implant are most often performed as outpatient surgery or with a single overnight stay at the Hospital for Special Surgery in New York. The exact plan depends on the procedure, your anesthesia, and your medical history, and is confirmed before your surgery date.
When can I return to work and sport after partial knee replacement?
Many patients with desk-based work return within 1–2 weeks while still using a cane; physically demanding jobs take longer. Recreational sport such as tennis, golf, and skiing in moderation is typically resumed by 3–6 months. MISHA recovery is faster — patients are usually off crutches within 2 weeks and back to most activities by 6–8 weeks. These are general ranges; your timeline depends on the procedure and your rehabilitation.
When can I drive after partial knee replacement?
Driving generally resumes by about 4 weeks for a right (operative) knee — sooner for a left knee with an automatic transmission — once you are off narcotic pain medication and can safely control the pedals. Confirm timing with Dr. Gomoll, and see our after-surgery instructions for the recovery milestones.
Does insurance cover partial knee replacement and MISHA?
Partial and total knee replacement are established procedures generally covered by insurance when medically necessary. The MISHA implant is FDA-cleared; coverage varies by plan and may require pre-authorization. Dr. Gomoll's administrative team handles approval — schedule a consultation for a personalized plan and a benefits check.
Dr. Gomoll evaluates and treats knee arthritis at the Hospital for Special Surgery, 523 East 72nd Street on Manhattan's Upper East Side, caring for patients from across New York City, the tri-state area, and beyond who want a compartment-sparing or joint-preserving option rather than moving straight to a total knee replacement. See our location and directions or request an appointment.
Medical disclaimer
This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Surgical and non-surgical orthopedic care should always be discussed with a board-certified orthopedic surgeon who has reviewed your imaging, history, and physical examination. Individual outcomes vary based on diagnosis, anatomy, comorbidities, and adherence to rehabilitation.