Cartilage repair helps restore damaged cartilage in the knee, relieve pain, improve function, and protect the joint from further wear. Cartilage injuries can result from sports injuries, accidents, repetitive stress, or conditions such as osteochondritis dissecans (OCD).
Dr. Gomoll offers some of the most advanced cartilage restoration procedures available, including MACI, osteochondral allograft transplantation (OCA), OATS, Cartiheal, DeNovo cartilage repair, and select stem-cell therapies through FDA-approved clinical trials. Every treatment plan is customized based on the size, location, and severity of the cartilage damage.
With more than 20 years of experience in cartilage restoration, Dr. Gomoll has performed over 1,000 MACI and OCA procedures. He also participated in the clinical research and FDA studies that helped bring many of these advanced treatments to patients across the United States.
What is cartilage repair?
Cartilage is the smooth tissue that covers the ends of bones where they meet to form a joint. In the knee, it allows the femur, tibia, and patella to move smoothly against one another during everyday activities.
Cartilage can be damaged by an injury, such as a sports injury, dislocation, or fall, by developmental conditions such as osteochondritis dissecans (OCD), or through gradual wear over time. A localized area of cartilage damage is called a focal cartilage defect, while more widespread cartilage loss is known as osteoarthritis.
Cartilage repair surgery is used to treat focal cartilage defects by restoring the damaged area of cartilage. The goal is to restore the joint surface and help delay or prevent progression to osteoarthritis. Patients with widespread bone-on-bone arthritis may be better candidates for other arthritis treatment options.
Who is a candidate for cartilage repair?
Most candidates have a focal cartilage defect visible on MRI, along with symptoms such as catching, locking, or pain during activity. Ideally, the ligaments and meniscus are healthy, although cartilage repair can often be combined with procedures to address these structures when needed. Dr. Gomoll evaluates four key factors when determining the best treatment approach:
Defect Size & Depth
The size and depth of the cartilage injury help determine which procedure is most appropriate. Smaller defects may be treated with DeNovo, OATS, or Cartiheal, while larger defects often require MACI or an osteochondral allograft.
Bone Involvement
In some patients, damage extends beyond the cartilage and into the underlying bone. When this occurs, an osteochondral allograft can restore both the bone and cartilage in a single procedure.
Alignment
The alignment of the leg affects how weight is distributed across the knee. Significant bow-legged (varus) or knock-kneed (valgus) alignment can place excess stress on the repair site. In these cases, an osteotomy may be recommended to protect the cartilage repair.
Meniscal Status
The meniscus acts as a shock absorber within the knee. If a significant portion of the meniscus is missing or damaged, a meniscal transplant may be recommended to improve the long-term durability of the cartilage repair.
How cartilage repair is performed
Dr. Gomoll offers several advanced cartilage restoration procedures. The best option depends on the size, location, depth, and characteristics of the cartilage injury.
01 Autologous Chondrocyte Implantation (MACI)

MACI is a two-stage procedure used to treat larger cartilage defects. During the first procedure, a small cartilage sample is collected arthroscopically. The cartilage cells are then grown in a specialized laboratory and placed onto a collagen membrane. Several weeks later, the membrane is implanted into the damaged area, where it helps restore the cartilage surface.
02 Osteochondral Allograft (OCA) Transplantation
OCA uses donor cartilage and bone to repair larger cartilage injuries. The graft is carefully matched to the size of the defect and implanted into the damaged area. This procedure is particularly useful when both the cartilage and underlying bone have been affected.
03 Particulated Cartilage Allograft (DeNovo)
DeNovo uses donor cartilage tissue to treat smaller cartilage defects. It is commonly used for cartilage injuries involving the kneecap (patella) and other smaller focal defects.
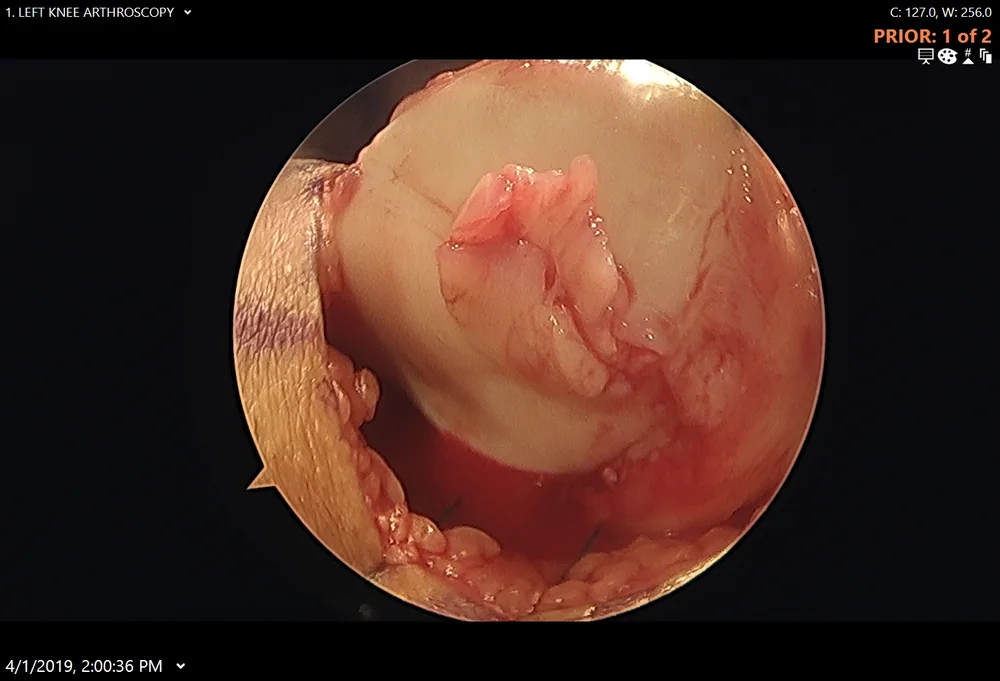 Before
Before 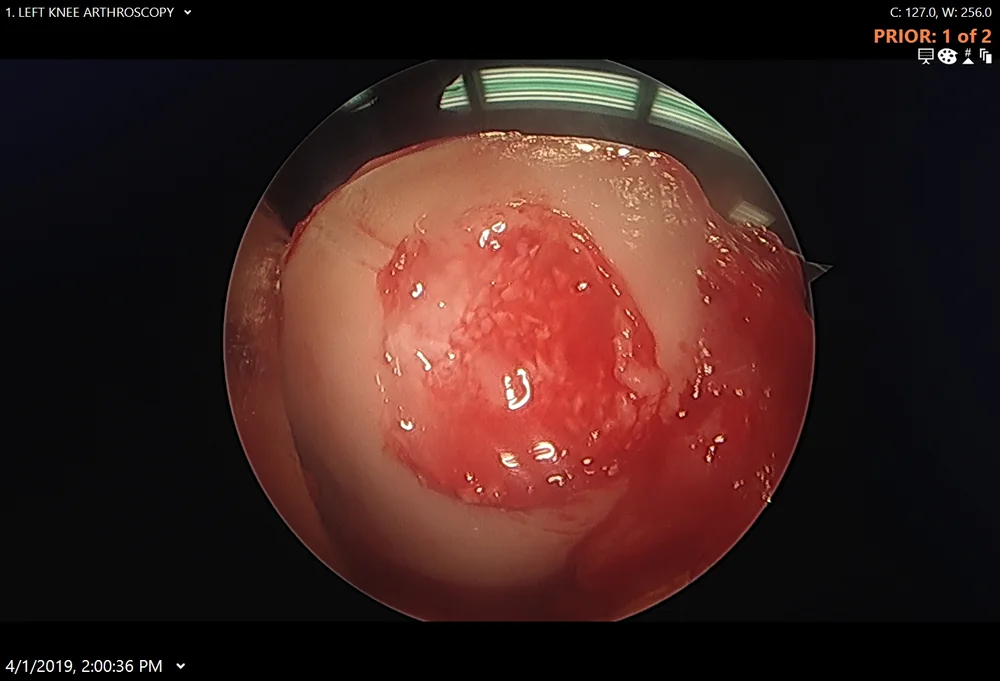 Finished graft
Finished graft 04 Autologous Osteochondral Transfer (OATS)
OATS uses healthy cartilage and bone from a less weight-bearing area of your own knee to repair a damaged area. Because it uses your own tissue, donor tissue is not required. This procedure is generally best suited for smaller cartilage defects.
05 Microfracture / Subchondral Drilling
Microfracture and subchondral drilling stimulate the body's natural healing response by creating small openings in the bone beneath the cartilage defect. This allows healing cells to enter the area and form repair tissue. These procedures are typically reserved for smaller cartilage injuries.
06 Umbilical Cord Mesenchymal Stem-Cell Transplantation (Cartistem® — Investigational)
Cartistem is an investigational cartilage restoration technique being studied through FDA-supervised clinical trials. The procedure combines specialized stem cells derived from donated umbilical cord blood with a supportive matrix that is placed into the cartilage defect to encourage cartilage repair.
07 Cartiheal Agili-C
An FDA-approved coral-based implant for small or oblong cartilage defects — including knees with mild degenerative changes that are otherwise not suitable for traditional cartilage repair. The Cartiheal Agili-C implant is made from sea coral, which is very similar to human bone in structure and composition. After it is implanted into the prepared defect, the coral scaffold gradually turns into bone while regenerating cartilage repair tissue on the surface. Because it is performed in a single stage, it does not require the two separate surgeries that staged techniques such as MACI involve. See the CBS New York story on Dr. Gomoll's use of the coral implant →
 Before
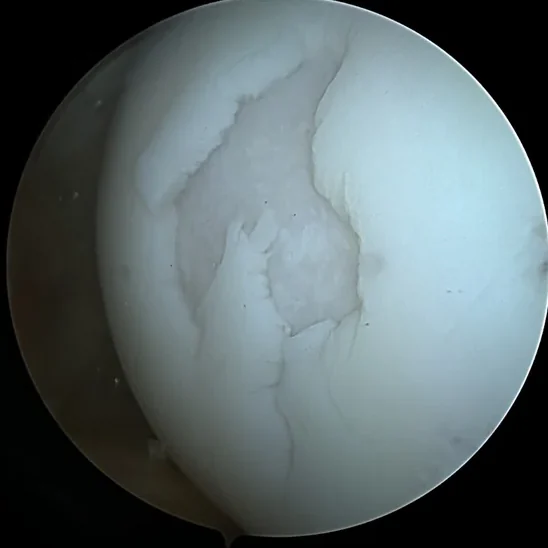
Before  1 year after
1 year after Imaging — before and after osteochondral allograft
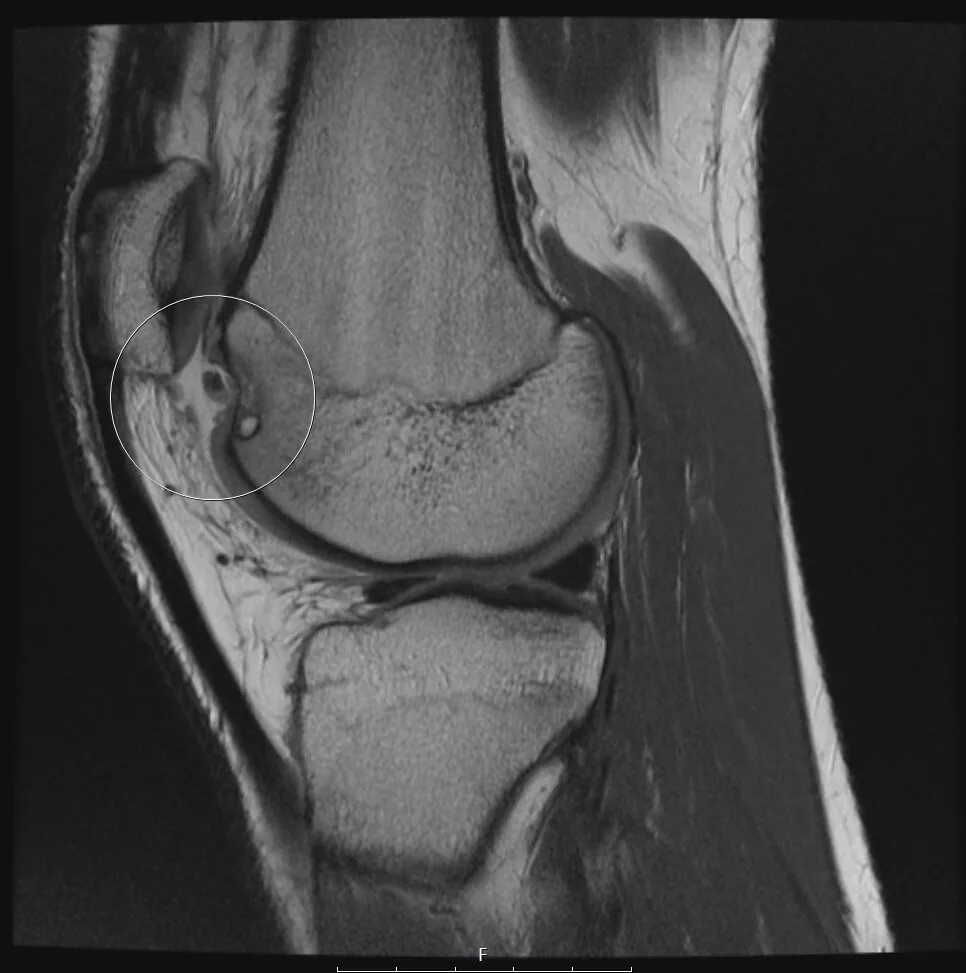 Before
Before  6 months after
6 months after For an additional patient-information sheet: Osteochondral allograft transplantation handout (PDF). For a procedure video: osteochondral allograft transplantation video.
Comparing the cartilage-repair techniques
There is no one-size-fits-all solution for cartilage damage. The best procedure depends on the size and location of the defect, whether the underlying bone is involved, and your individual goals and activity level. The table below provides a general overview of the most commonly used cartilage restoration techniques.
| Technique | Best suited for | Tissue used | Staged? | Repair tissue |
|---|---|---|---|---|
| Microfracture / subchondral drilling | Smaller defects (generally under ~2 cm²) | None — your own bone-marrow elements | No — single arthroscopic procedure | Fibrocartilage (weaker than native cartilage) |
| MACI (autologous chondrocyte implantation) | Larger defects on the femoral condyle, trochlea, or patella with healthy underlying bone | Your own chondrocytes grown on a collagen membrane | Yes — two procedures, 4–6 weeks apart | Hyaline-like cartilage |
| Osteochondral allograft (OCA) | Larger defects, especially when the bone beneath the cartilage is also damaged (e.g. advanced OCD) | Size-matched donor bone and cartilage (no anti-rejection medication needed) | No — single procedure | Mature donor hyaline cartilage |
| OATS / mosaicplasty | Small-to-mid defects where enough graft can be harvested | Your own osteochondral plugs from a less weight-bearing area of the same knee | No — single procedure | Your own hyaline cartilage |
| Cartiheal Agili-C | Small or oblong defects, even in the setting of mild osteoarthritis | Sea coral, which is very similar to human bone in structure and composition — it turns into bone while regenerating cartilage repair tissue | No — single procedure | Hyaline-like cartilage |
| Umbilical-cord MSC transplant (Cartistem® — investigational) | Selected patients enrolled in the FDA-supervised clinical trial | Umbilical-cord-blood mesenchymal stem cells mixed with hyaluronan | No — single procedure | Cartilage matured from implanted stem cells |
Why the Distinction Matters: Not all cartilage repair procedures produce the same type of repair tissue. Microfracture stimulates the body to form fibrocartilage, while procedures such as MACI, OCA, and OATS are designed to restore cartilage that more closely resembles the knee's natural cartilage. This is one reason why larger defects and injuries involving the underlying bone often require a graft-based procedure rather than microfracture alone.
Dr. Gomoll's approach to cartilage repair
The most important decision in cartilage repair is choosing the right procedure for the specific defect. For smaller cartilage defects with healthy underlying bone, subchondral drilling is often a good starting point because it is a minimally invasive arthroscopic procedure performed in a single surgery.
However, not every defect can be treated this way. When the damaged area is larger, or when the bone beneath the cartilage is also affected — as is often the case in advanced osteochondritis dissecans (OCD) — an osteochondral allograft is often preferred because it restores both the cartilage surface and the underlying bone in a single procedure.
Dr. Gomoll also treats the entire knee, not just the cartilage defect. Problems such as poor alignment, meniscus deficiency, or ligament instability can place extra stress on a cartilage repair and reduce its long-term durability. When necessary, procedures such as an osteotomy or meniscal transplant may be performed at the same time to create the best environment for healing.
The goal of joint preservation is to restore and protect the patient's natural joint surface, helping to delay or avoid joint replacement whenever possible.
Preparing for cartilage repair surgery
Pre-operative preparation includes high-resolution MRI (preferably HSS quality — see our imaging page), a focused clinical exam, and review of medical history and prior knee surgery. Patients stop narcotics 14 days before surgery and blood thinners or supplements that increase bleeding risk 7–10 days before. Nothing by mouth after midnight on the surgical date.
Insurance pre-authorization is handled by Dr. Gomoll's administrative team — see our before-surgery checklist for the full pre-op timeline. For day-of-surgery logistics, see what to expect on the day of surgery.
Anesthesia & staying comfortable
Cartilage repair is performed under general or spinal anesthesia, usually paired with a regional nerve block that keeps the leg numb well after you wake up — so most patients are surprised how manageable the first day is.
You will meet your anesthesiologist before surgery to choose the approach that fits you. A regional block typically lasts about 6–8 hours after the procedure, smoothing the transition home. Most cartilage-repair procedures are outpatient or a single overnight stay, and most patients move to oral pain medication within the first day or two and rely on it for only the first 1–2 weeks.
Worried about pain medication? The goal is to control pain with the lowest effective amount of medication for the shortest time, supported by ice, elevation, and the nerve block — not to leave you dependent on opioids. The exact plan and timeline are in our after-surgery instructions, and bracing and cold-therapy options are covered on our bracing & ice machine page.
Risks to understand
Cartilage repair is a joint-preservation surgery with a strong track record, but like any operation it carries risks you should weigh with Dr. Gomoll before deciding. Depending on the technique, these can include infection, blood clots (DVT/PE), knee stiffness or arthrofibrosis, incomplete graft integration or failure of the repair to fill the defect, and progression of arthritis over time. Marrow-stimulation techniques such as microfracture form fibrocartilage that is biomechanically weaker than native cartilage and can break down in larger or high-demand defects. The umbilical-cord stem-cell technique is investigational and does not have a guaranteed outcome.
No cartilage procedure is a guaranteed permanent fix. These techniques are designed to relieve pain, restore the joint surface, and delay or avoid joint replacement — but results depend on defect size and location, alignment, body weight, activity level, and how closely you follow the rehabilitation protocol. Dr. Gomoll will review the specific risks and realistic expectations for your knee at your consultation.
Materials & technologies we use
- Vericel MACI — FDA-approved autologous chondrocyte implantation system using your own cartilage cells grown on a porcine collagen membrane
- Fresh osteochondral allograft from FDA-regulated tissue banks — size-matched donor bone-and-cartilage cylinders
- Smith & Nephew Cartiheal Agili-C coral implant — FDA-approved cartilage-repair implant for the treatment of patients with mild degenerative changes otherwise not suitable for cartilage repair. See an interview with Dr. Gomoll regarding its use.
- Cartistem® — umbilical-cord-blood mesenchymal stem cells (FDA-supervised clinical trial)
- Arthroscopic instrumentation — high-definition fiber-optic camera, motorized shavers, dedicated cartilage-prep instruments
- HSS imaging — high-resolution 3T MRI for defect mapping and surgical planning
Follow-up & long-term outcomes
Recovery depends on the technique:
Microfracture / subchondral drilling
6 weeks protected weight-bearing on crutches; 6–12 weeks PT focused on early range of motion and progressive loading.
MACI
6–8 weeks non-weight-bearing or partial weight-bearing after the implantation procedure; phased PT advancing over 6–12 months.
Osteochondral allograft
6–8 weeks protected weight-bearing while bone integrates; PT phases advance over 6–9 months; full activity by 9–12 months.
OATS
Early range of motion, partial weight-bearing for 4–6 weeks, return to sport by 6–9 months.
Detailed phase-by-phase PT plans for each technique are downloadable on our knee rehab protocols page. General recovery timelines (driving, work, showering) are on our after-surgery FAQ.
Documented case studies from our practice
Real cartilage-repair cases with intra-operative photographs, technique rationale, and outcomes:
- Patrick — back racing Ironman after a cartilage transplant — osteochondral allograft plus cadaver ACL reconstruction in an endurance athlete who had been told he needed a knee replacement
- Pamela — osteochondral allograft transplantation — a joint-preserving OCA for a focal knee cartilage defect, chosen over early knee replacement
- Fresh osteochondral allograft — CrossFit & football athlete — a recurrent defect after a failed reattachment, definitively treated with a size-matched donor plug
- Subchondral drilling case (intra-operative) — a focal defect in the medial femoral condyle treated with marrow-stimulation drilling
- Umbilical-cord MSC implantation case (intra-operative) — a medial femoral condyle defect treated with mesenchymal stem cells from umbilical-cord blood (Cartistem® trial)
More written outcomes are on our patient testimonials page.
Frequently asked questions
How long does cartilage repair surgery take?
It depends on the technique. Microfracture / subchondral drilling is the fastest (often performed during a diagnostic arthroscopy and adding 30–45 minutes). MACI is staged across two procedures separated by 4–6 weeks. Osteochondral allograft transplantation typically takes 1–2 hours depending on defect size and location.
Is cartilage repair painful?
Procedures are performed under general or spinal anesthesia, often combined with a regional nerve block that lasts 6–8 hours after surgery. Most patients are discharged the same day or next morning and use oral pain medication for the first 1–2 weeks. See our after-surgery instructions for the typical pain-control timeline.
Am I a candidate for cartilage repair?
Candidates typically present with a focal cartilage defect (a localized area of damage) rather than diffuse arthritis. Dr. Gomoll uses high-resolution MRI — preferably from HSS — to assess defect size, depth, location, and surrounding bone integrity. Patients with significant malalignment may need a concurrent osteotomy; patients with bone loss may need an osteochondral allograft instead of a soft-tissue technique like MACI.
What materials are used?
MACI uses your own chondrocytes grown on a porcine collagen membrane (Vericel MACI). Osteochondral allografts use cadaver donor bone-and-cartilage matched to your defect size. OATS uses your own osteochondral plugs from a less weight-bearing area of the same knee. Microfracture / subchondral drilling uses no implant — only your bone marrow elements.
How much does cartilage repair cost, and does insurance cover it?
Cost varies based on technique, anesthesia, operating-room time, implant cost, and your insurance. Established techniques such as MACI, osteochondral allograft, OATS, and microfracture are generally covered when medically necessary; some advanced techniques may require an appeal, and the investigational umbilical-cord stem-cell technique is handled through the clinical trial. Insurance pre-authorization is managed by Dr. Gomoll's administrative staff before surgery — schedule a consultation for a personalized plan and a benefits check.
Is cartilage repair outpatient or inpatient?
Most cartilage-repair procedures are performed as outpatient surgery or with a single overnight stay at the Hospital for Special Surgery in New York. The exact plan depends on the technique, your anesthesia, and your medical history, and is confirmed before your surgery date.
When can I return to work and sport after cartilage repair?
Recovery depends on the technique and your job. Many patients with desk-based work return within 1–2 weeks while still on crutches; physically demanding jobs take longer. Return to recreational activity is typically around 6–9 months and full sport around 9–12 months for graft procedures such as MACI and osteochondral allograft. These are general ranges — your timeline depends on your defect, the procedure, and your rehabilitation.
When can I drive after cartilage repair?
Driving generally resumes once you are off crutches and narcotic pain medication and can safely control the pedals — often a few weeks for the operative leg, sooner if it is the non-driving leg. Confirm timing with Dr. Gomoll, and see our after-surgery instructions for the recovery milestones.
Dr. Gomoll evaluates and treats cartilage defects of the knee at the Hospital for Special Surgery, 523 East 72nd Street on Manhattan's Upper East Side, caring for patients from across New York City, the tri-state area, and beyond who want to preserve their own joint rather than move straight to replacement. See our location and directions or request an appointment.
Medical disclaimer
This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Surgical and non-surgical orthopedic care should always be discussed with a board-certified orthopedic surgeon who has reviewed your imaging, history, and physical examination. Individual outcomes vary based on diagnosis, anatomy, comorbidities, and adherence to rehabilitation.