The meniscus is a C-shaped piece of cartilage that acts as a shock absorber between the femur and tibia in the knee. When the meniscus tears, treatment may include removing the damaged portion (partial meniscectomy), repairing the tear with sutures, or, in select patients who have previously lost significant meniscal tissue, meniscal transplantation.
Whenever possible, Dr. Gomoll focuses on preserving and repairing the meniscus to help protect the knee cartilage and support long-term joint health.
What are meniscal procedures?
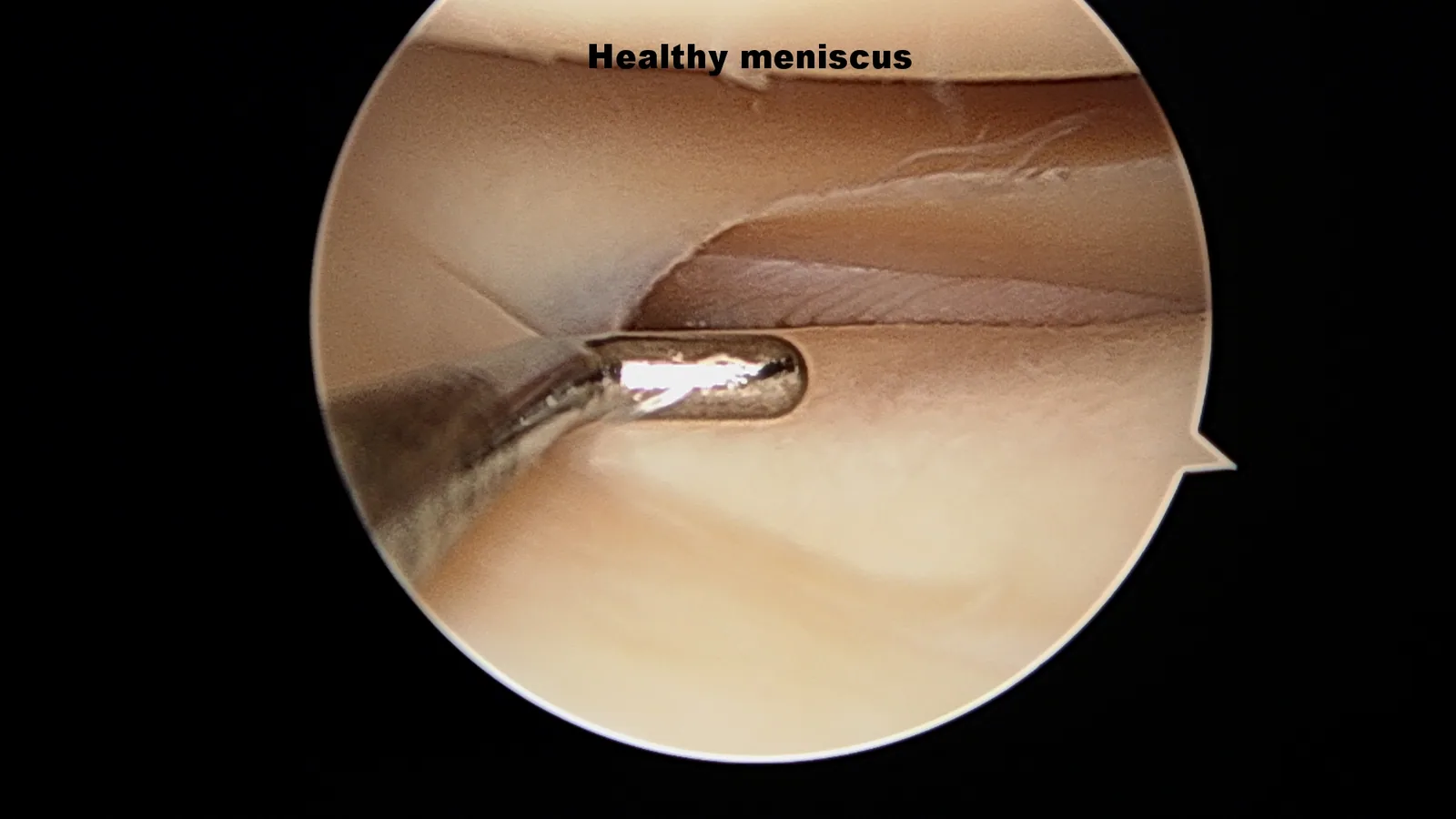
The meniscus is a horseshoe-shaped piece of fibrocartilage between the articular surfaces of the femur and tibia. There are two menisci in each knee — a medial and a lateral — and each acts as a shock absorber, distributes load, and stabilizes the joint. The meniscus is frequently damaged through acute injury (cutting, pivoting, deep flexion under load) or chronic degeneration. Dr. Gomoll discusses meniscus preservation in this video.
Meniscal tears are treated with one of three approaches: partial meniscectomy (removing the torn portion), meniscal repair (suturing the tear so it heals), or — for patients with prior near-total meniscectomy and persistent symptoms — meniscal allograft transplantation (replacing the missing meniscus with donor tissue).
Who is a candidate for meniscal surgery?
Indications depend on the procedure:
- Meniscectomy: patients with mechanical symptoms (catching, locking, sharp pain with pivoting) from a torn meniscus that cannot be repaired (e.g., complex degenerative tears, tears in the avascular inner zone)
- Meniscal repair: patients with tears in the vascular outer zone of the meniscus, particularly bucket-handle, vertical, or peripheral tears with healthy surrounding tissue. Younger, more active patients are best candidates
- Meniscal transplantation: patients with prior near-total meniscectomy who develop activity-related pain and swelling, before bone-on-bone arthritis sets in. Concurrent ligament reconstruction or osteotomy may be needed if alignment or ACL function is compromised
For patients with combined meniscal and cartilage damage, Dr. Gomoll often performs meniscal repair or transplantation alongside cartilage repair in a single procedure.
When meniscus surgery may not be the answer: not every meniscus tear needs an operation. Many degenerative tears in older patients with early arthritis improve with physical therapy, activity modification, and time — and surgery on a degenerative tear in an arthritic knee may not relieve pain. Meniscal transplantation is not appropriate once bone-on-bone arthritis has already developed, and outcomes are poorer in patients with significant cartilage loss, uncorrected malalignment, or untreated ligament instability. Dr. Gomoll will discuss whether a non-surgical course or a staged plan is the better starting point for your knee.
How meniscal surgery is performed
Three approaches, selected to preserve as much healthy meniscus as possible. Expand each for a demonstration video and intra-operative images.
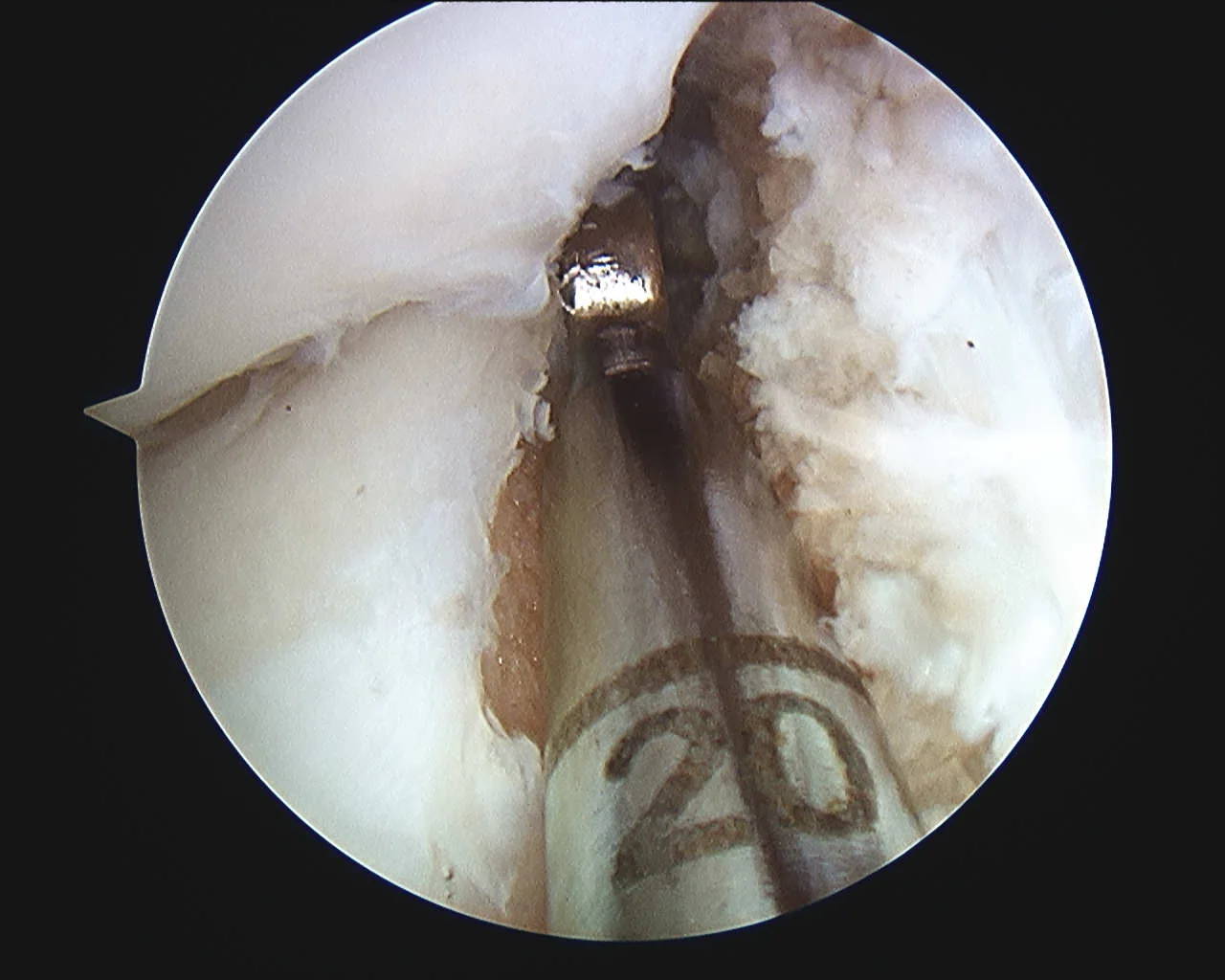
1 Meniscectomy (partial removal)
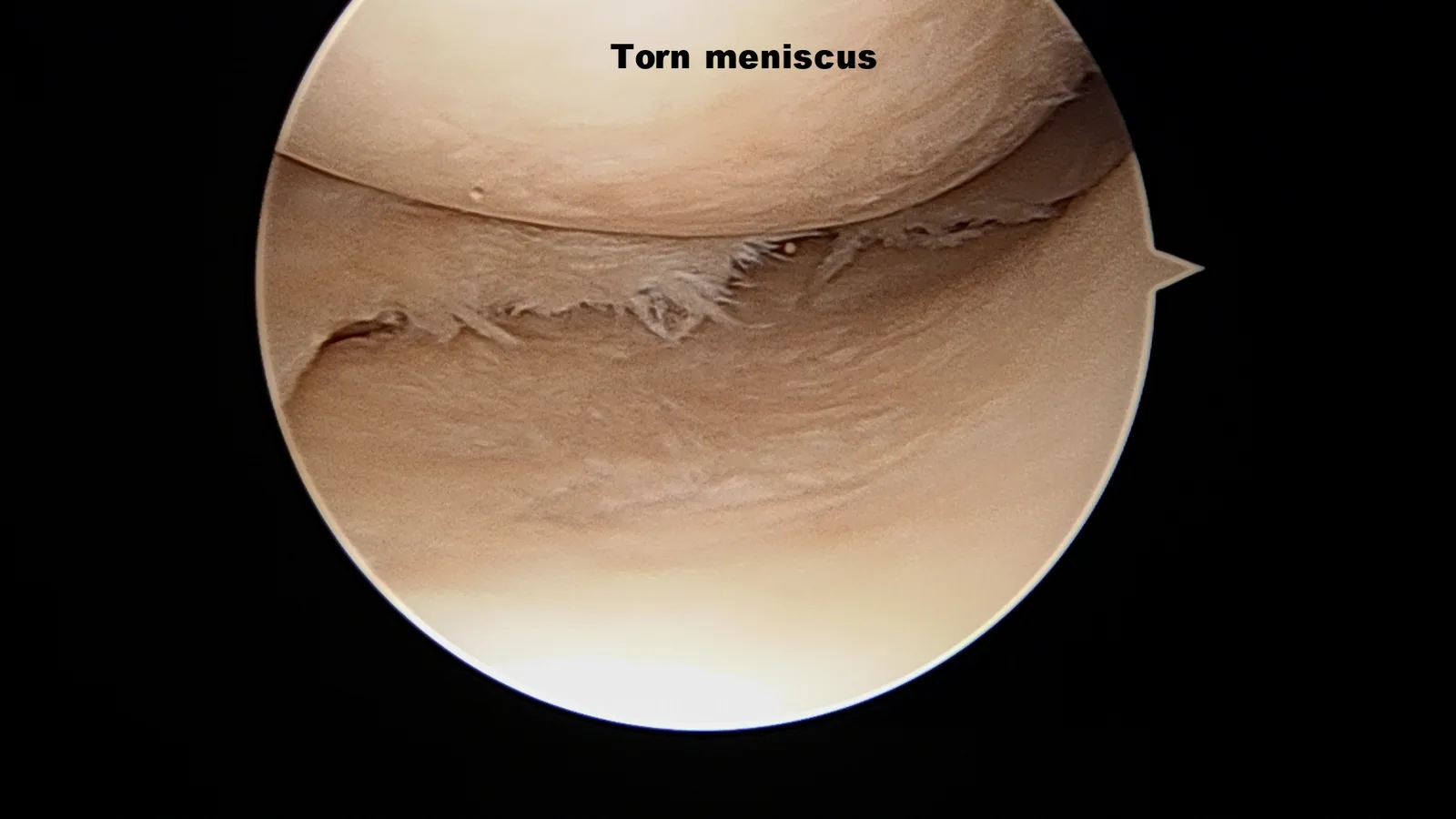
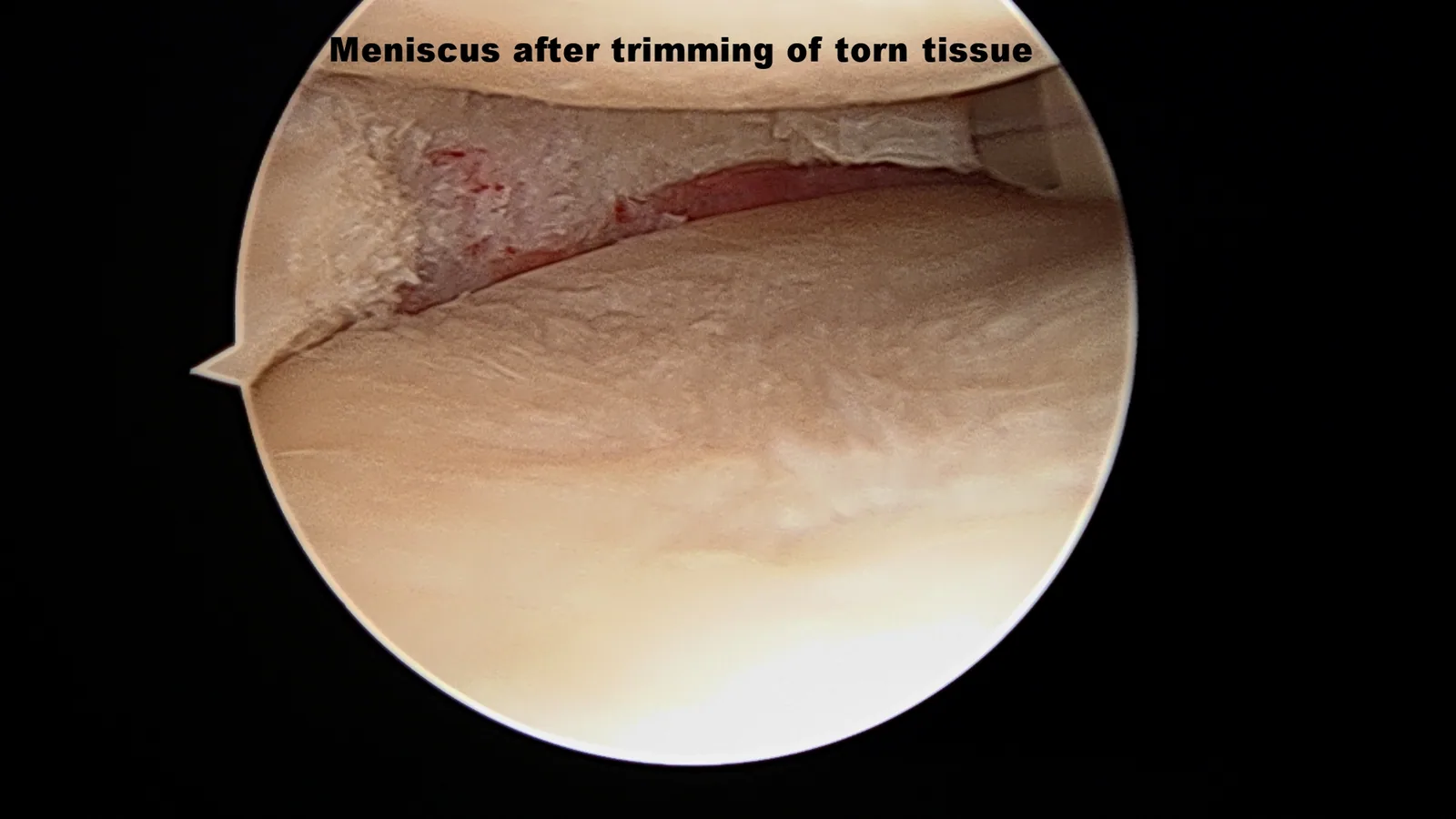
By far the most common meniscal procedure (>90% of meniscal surgery), meniscectomy refers to removal of unstable torn meniscus tissue causing symptoms. During this arthroscopic procedure, a fiber-optic camera is inserted through small portal incisions and the torn portion is removed with a motorized shaver, leaving as much healthy tissue behind as possible.

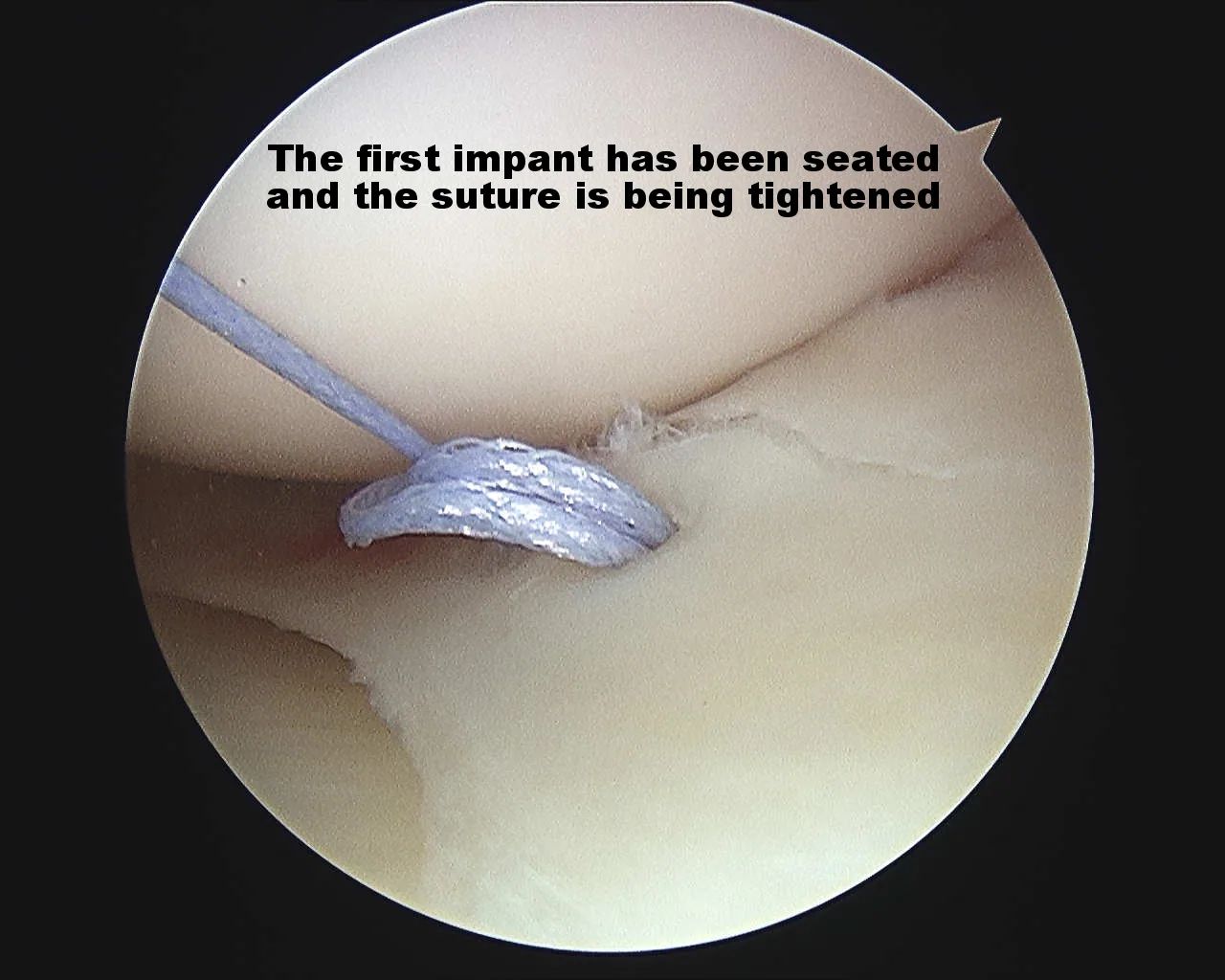
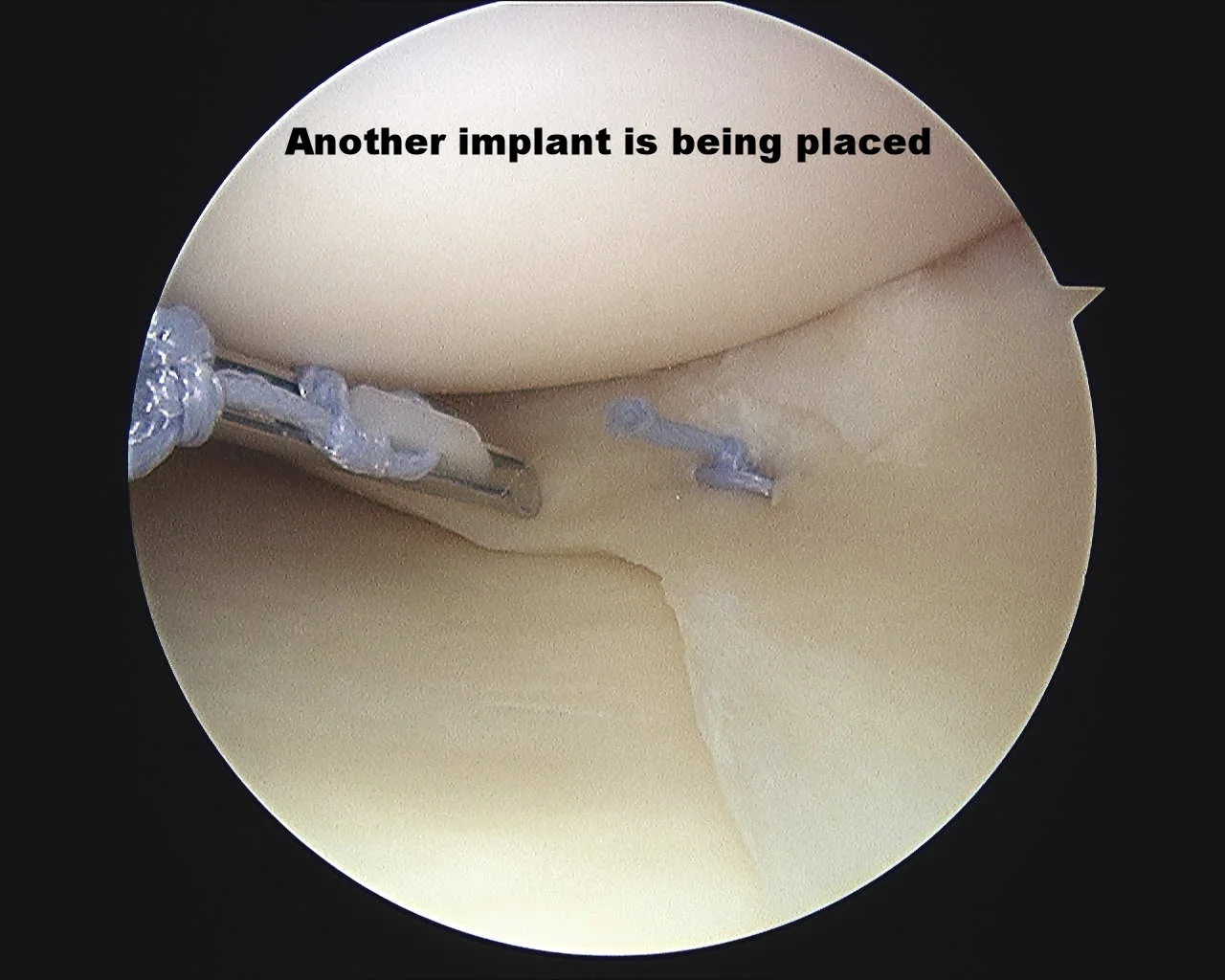
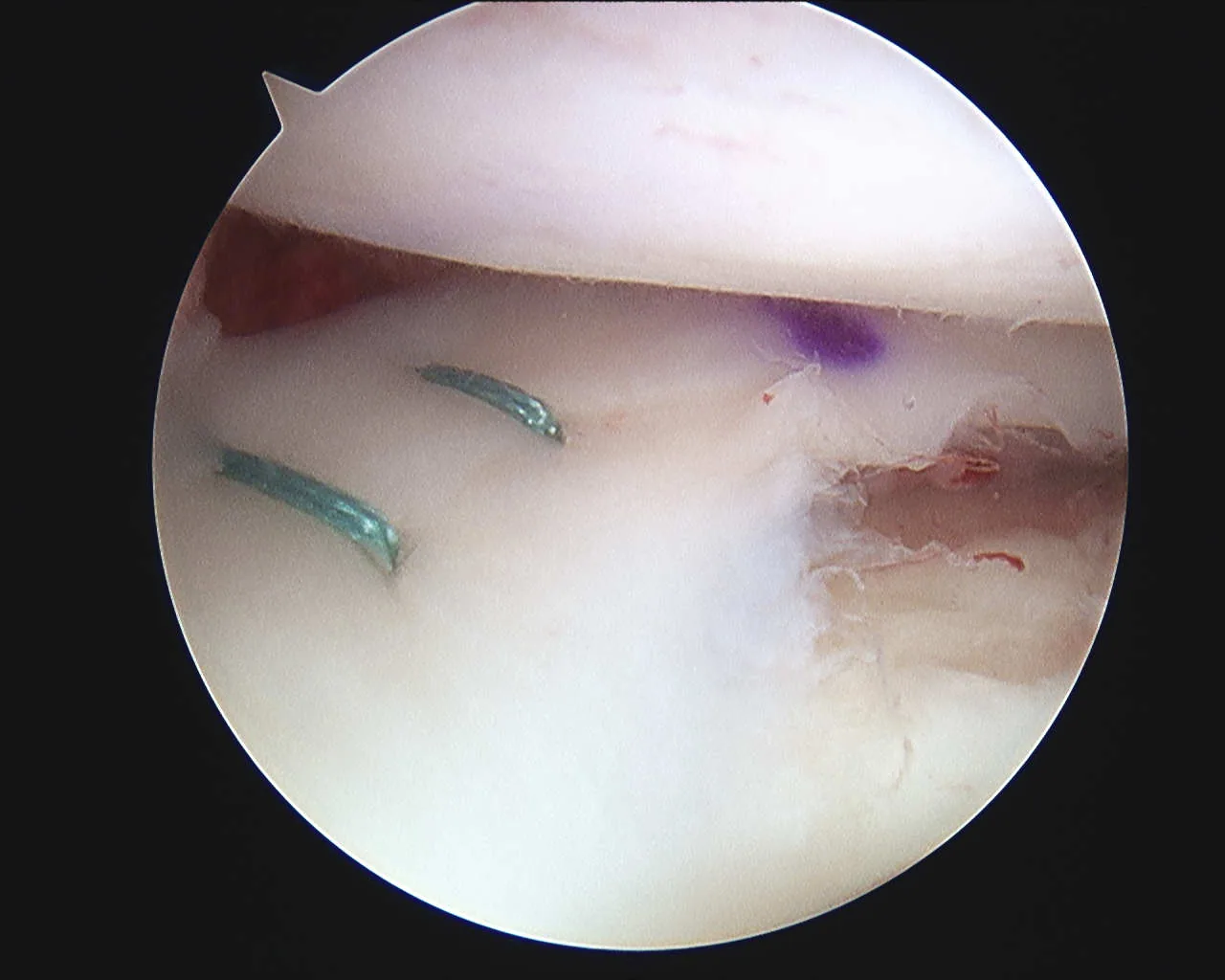
2 Meniscal repair
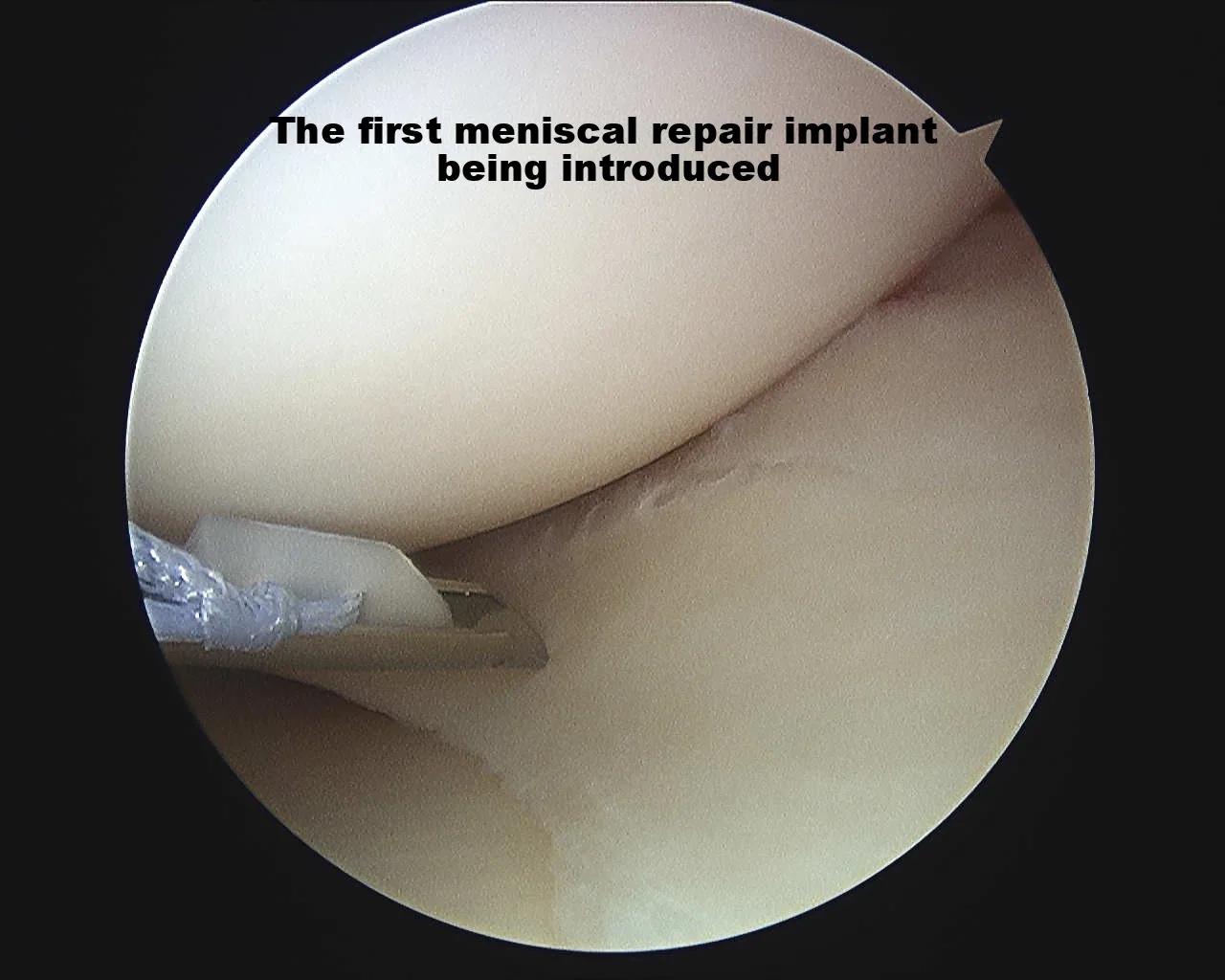
For repairable tears (most often bucket-handle or peripheral vertical tears in the vascular outer zone), the torn meniscus is arthroscopically reduced and stabilized with all-inside suture anchors or inside-out / outside-in suture techniques. Without repair, an unstable bucket-handle tear can lock the knee and cause further tearing. After repair with several suture devices, the meniscus is stable to probing. The need for crutches depends on the tear type, ranging from 2–6 weeks.

3 Meniscal allograft transplantation
When a meniscus has been previously removed and the patient develops symptoms of meniscal deficiency, transplantation can be considered. Donor meniscal tissue is size-matched, cleaned, and frozen by a transplant organization, then shipped to the hospital before the procedure.
During surgery, Dr. Gomoll arthroscopically removes any non-functional remnants of the prior meniscus, prepares the joint, and introduces the new meniscus through a small front incision. The graft is repaired to the tibia (often with bone fixation at the anterior and posterior horns) and sutured to the joint capsule through a second small incision on the side of the knee.

Repair vs. removal vs. transplant
The right meniscus operation depends on the tear pattern, its location relative to the blood supply, and how much healthy tissue remains. Dr. Gomoll matches the technique to the tear, preserving as much native meniscus as possible. This table summarizes how the three approaches differ.
| Approach | Best suited for | What happens to the meniscus | Weight-bearing after surgery | Return to sport |
|---|---|---|---|---|
| Partial meniscectomy | Complex or degenerative tears, and tears in the avascular inner "white zone" that cannot heal | The unstable torn portion is trimmed away; healthy tissue is preserved | Full weight-bearing immediately | ~4–6 weeks |
| Meniscal repair | Bucket-handle, vertical, or peripheral tears in the vascular outer "red zone," especially in younger, active patients | The tear is sutured so the meniscus heals and is retained | Protected weight-bearing with crutches and brace for 4–6 weeks | ~4–6 months |
| Meniscal allograft transplantation | Prior near-total meniscectomy with symptoms of meniscal deficiency, before bone-on-bone arthritis develops | The missing meniscus is replaced with size-matched donor tissue | Protected weight-bearing with crutches and brace for 4–6 weeks | ~6–9 months |
Why preserving the meniscus matters: the meniscus distributes load and protects the articular cartilage. Removing more tissue than necessary increases contact stress on the cartilage and can accelerate arthritis over time — which is why repair is favored whenever the tear pattern and tissue quality allow it, and why transplantation is offered to selected patients before arthritis sets in.
Dr. Gomoll's approach to meniscal surgery
Dr. Gomoll selects the treatment based on the type of tear and the condition of the meniscal tissue rather than automatically removing the damaged portion. Because the meniscus plays an important role in absorbing shock and protecting the knee cartilage, every effort is made to repair a tear whenever possible — especially in younger, active patients and in tears located in the outer portion of the meniscus where healing potential is greater.
When a tear cannot be repaired, only the damaged and unstable portion is removed while preserving as much healthy meniscal tissue as possible.
Dr. Gomoll also evaluates the entire knee, not just the meniscus tear. When meniscal deficiency occurs alongside malalignment, ligament instability, or cartilage damage, those issues may need to be addressed as part of the treatment plan. Depending on the findings from the examination and imaging studies, a meniscal transplant may be performed alone or combined with an osteotomy, ligament reconstruction, or cartilage repair procedure to create the best environment for long-term success.
Preparing for meniscal surgery
Pre-operative preparation includes MRI to confirm tear location and configuration, a focused clinical exam, and review of medical history. Patients stop narcotics 14 days before, blood thinners and supplements that increase bleeding risk 7–10 days before, and nothing by mouth after midnight on the surgical date. See our before-surgery checklist for the full timeline.
Imaging quality matters — review our imaging page for guidance.
Anesthesia & staying comfortable
Meniscal surgery is performed under general or spinal anesthesia, paired with long-lasting local anesthesia or occasionally a regional nerve block that helps the pain for 24–36 hours.
You will meet Dr. Gomoll and your anesthesiologist before surgery to choose the approach that fits you. Arthroscopic meniscus procedures, including transplantation, are outpatient procedures. Many meniscectomy patients only require anti-inflammatories, Tylenol and ice; meniscus repair and transplant patients may use narcotic pain medication for the first 2–3 days in addition.
Worried about pain medication? The goal is to control pain with the lowest effective amount of medication for the shortest time, supported by ice, elevation, and the long-lasting local pain-medication injection — not to leave you dependent on opioids. The full pain-control timeline is in our after-surgery instructions, and bracing and cold-therapy options are covered on our bracing & ice machine page.
Common concerns about meniscus surgery
"Will my insurance cover it?"
Meniscectomy and standard meniscal repair are typically covered when medically necessary. Meniscal transplantation may require a more detailed authorization, sometimes including an appeal — Dr. Gomoll's administrative team manages pre-authorization before surgery.
"How long will recovery take?"
A meniscectomy is among the faster knee recoveries — many patients return to desk work within a few days and everyday activities within 1–2 weeks. Repair and transplant trade a longer recovery for the long-term benefit of keeping a working meniscus.
"I'm nervous about the surgery itself."
Most meniscal surgery is arthroscopic — performed through small portal incisions with a camera — and done as a same-day outpatient procedure. Dr. Gomoll will walk you through exactly what to expect at your consultation.
Risks to understand
Meniscal surgery is common and generally well tolerated, but like any operation it carries risks you should weigh with Dr. Gomoll before deciding. Depending on the procedure, these can include infection, blood clots (DVT/PE), knee stiffness, a repaired or transplanted meniscus that does not fully heal and may re-tear, and progression of arthritis over time — particularly when meniscal tissue has been removed. Because meniscal repair and transplantation rely on biological healing, a second procedure is sometimes needed if the tissue fails to heal.
No meniscus procedure is a guaranteed permanent fix. These operations are designed to relieve mechanical symptoms, protect the cartilage, and restore function — but results depend on the tear pattern, tissue quality, alignment, body weight, activity level, and how closely you follow the rehabilitation protocol. Dr. Gomoll will review the specific risks and realistic expectations for your knee at your consultation.
Materials & technologies we use
- All-inside meniscal repair devices — rapid, low-profile suture anchors that minimize neurovascular risk
- Inside-out / outside-in suturing for tears in zones not accessible with all-inside devices
- Suture passing devices such as Knee Scorpion, Novostitch, FirstPass
- ActivBraid Collagen co-braid suture to improve biologic healing rates
- Fresh-frozen meniscal allografts from FDA-regulated tissue banks — size-matched to within ±5% of native dimensions
- Arthroscopic instrumentation — high-definition fiber-optic camera, motorized shavers, biters, dedicated meniscal-repair instruments
- HSS imaging — high-resolution 3T MRI for tear identification and surgical planning
Follow-up & long-term outcomes
Meniscectomy
Full weight-bearing immediately, PT focused on swelling control and quad activation in week 1, return to running at 4 weeks and sport at 4–6 weeks.
Meniscal repair
Protected weight-bearing in a brace for 4–6 weeks with controlled ROM, progressive loading 6–12 weeks, return to sport at 4–6 months.
Meniscal transplantation
Protected weight-bearing in a brace for 4–6 weeks, generally followed by an additional 6 weeks in a compartment-unloading brace to protect the transplant while allowing weight-bearing as tolerated, phased PT over 6–9 months, return to impact activity at 6–9 months.
Phase-by-phase PT plans are downloadable on our knee rehab protocols page. General recovery FAQs are on our after-surgery page.
Patient outcomes
Real outcomes from Dr. Gomoll's meniscal practice:
- KN — meniscus transplantation + distal femoral osteotomy — high-school athlete back to competitive cross-country and indoor track
- AD — distal femoral osteotomy + lateral meniscal allograft transplantation — meniscal-deficient knee treated with a combined transplant and realignment
- Jennifer — HTO + ACL reconstruction — a combined realignment-and-ligament case in a volleyball player, the kind of multi-structure plan that protects a meniscus transplant or repair
- Documented intra-operative cases — arthroscopic photographs from related meniscal and cartilage cases
- Research: Anatomic risk factors for cartilage lesions — American Journal of Sports Medicine, 2019
More written outcomes are on our patient testimonials page.
Frequently asked questions
How long does meniscus surgery take?
Arthroscopic meniscectomy typically takes 30–45 minutes; meniscal repair adds 30–60 minutes depending on tear configuration; meniscal transplantation takes approximately 2 hours due to graft preparation and fixation.
Is meniscus surgery painful?
Procedures are performed under general or spinal anesthesia, frequently with additional local anesthetic lasting 6–8 hours after surgery. Patients are discharged the same day. Meniscectomy patients typically use only anti-inflammatories, ice and Tylenol after the first 2–3 days; repair and transplant patients may need narcotic pain medication for 2–3 days in addition.
Can my meniscus tear be repaired or does it need to be removed?
It depends on tear location, configuration, and tissue quality. Tears in the vascular outer "red zone" of the meniscus can heal and are repaired. Tears in the avascular inner "white zone," complex degenerative tears, and chronic tears with frayed tissue typically require partial removal (meniscectomy). Dr. Gomoll preserves as much healthy meniscus as possible — every effort is made to repair before resorting to meniscectomy.
What is meniscus transplantation and who needs it?
Meniscal transplantation replaces a missing or non-functional meniscus with size-matched donor tissue. It is considered for patients with prior near-total meniscectomy who develop activity-related pain and swelling from meniscal deficiency, before bone-on-bone arthritis develops. Outcomes are best in younger, active patients with intact ligaments and minimal cartilage damage.
How much does meniscus surgery cost?
Cost varies by procedure, anesthesia, and your insurance. Meniscectomy and standard meniscal repair are typically covered without difficulty when medically necessary; meniscal transplantation may require a more detailed insurance authorization, sometimes including an appeal. Dr. Gomoll's administrative team handles approval — see our before-surgery insurance page, or schedule a consultation for a personalized plan and a benefits check.
Is meniscus surgery outpatient or inpatient?
Meniscectomy, meniscal repair, and meniscal allograft transplantation are typically performed as outpatient surgery at the Hospital for Special Surgery in New York — most patients go home the same day. The exact plan depends on the procedure, your anesthesia, and your medical history, and is confirmed before your surgery date.
When can I return to work and sport after meniscus surgery?
Recovery depends on the procedure. Meniscectomy patients often return to desk work within a few days, to most everyday activities within 1–2 weeks, and recreational sport at 4–6 weeks. Meniscal repair requires a brace and protected weight-bearing for 4–6 weeks, with return to sport around 4–6 months while the tear heals. Meniscal transplantation is the longest, with phased rehabilitation over 6–9 months before impact activity. These are general ranges — your timeline depends on the tear, the procedure, and your rehabilitation.
When can I drive after meniscus surgery?
Many meniscectomy patients drive within a few days to a week once able to walk comfortably and control the pedals safely. Repair and transplant patients in a brace with protected weight-bearing wait longer — often several weeks for the operative leg. Confirm timing with Dr. Gomoll, and see our after-surgery instructions for the recovery milestones.
Dr. Gomoll evaluates and treats meniscus tears and meniscal deficiency at the Hospital for Special Surgery, 523 East 72nd Street on Manhattan's Upper East Side, caring for patients from across New York City, the tri-state area, and beyond who want to preserve their own meniscus and cartilage rather than move straight to replacement. See our location and directions or request an appointment.
Medical disclaimer
This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Surgical and non-surgical orthopedic care should always be discussed with a board-certified orthopedic surgeon who has reviewed your imaging, history, and physical examination. Individual outcomes vary based on diagnosis, anatomy, comorbidities, and adherence to rehabilitation.